COVID-19 has killed over 220,000 Americans, including my cousin.
At 31, Marny had just started her tenure as Chair of the Saint Paul School Board. She was intelligent, beautiful, and ambitious, but most of all, she was kind and compassionate. While I was often a wallflower, Marny always dazzled the room. At family reunions and community gatherings, she would easily maneuver between Hmong and English, bring the young and the old together in conversation, and discuss why our communities needed to work within and without to progress the rights of all students.
In the days leading up to her death, she was a shell of her former self. She could not speak or laugh; the only sounds emitting from the screens of our laptops were the cries of our family and the humming of the ventilator breathing for her. Her death devastated my family. Marny and her father were admitted to the emergency room at separate hospitals on the same day, and while he survived, my uncle continues to experience complications from the virus. His COVID-19 treatment cost over $200,000. While his health insurance covered his treatment, many uninsured Americans will survive this pandemic, endure prolonged health effects, and face an insurmountable financial hurdle.
On Nov. 10, the Supreme Court will hear oral arguments in California v. Texas, a case seeking to strike down the Affordable Care Act (ACA) led by 20 Republican state attorney generals with the backing of the Trump Administration. If the Court decides to repeal the ACA, 20 million people will lose their health insurance, and millions more will be at risk of losing or being denied coverage due to pre-existing conditions, which may eventually encompass COVID-19.
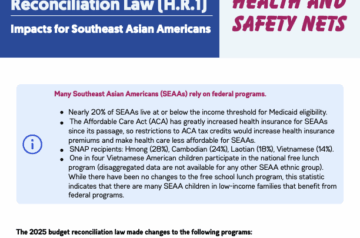
According to the Census Bureau, the uninsured population in the United States increased from 8.9% in 2018 to 9.2% in 2019, meaning an additional one million people became uninsured last year. Similarly, the uninsured Cambodian, Hmong, and Vietnamese population also increased in 2019, with a 0.8% uptick among Cambodians, 0.6% among Hmong, and 1% among Vietnamese Americans. In spite of this data and the pandemic, the Administration continues to support the repeal of the ACA. Officials even shortened the open enrollment period for 2021 from 90 days to 45 days, which opens on Nov. 1 and ends on Dec. 15, 2020. This pandemic has taught us that our country needs to protect the ACA and expand healthcare access, not strip insurance from millions of people.
Isolated, unable to speak English, and recovering from a speech impediment due to a prior stroke, our grandmother could barely ask for water and couldn’t even request food or to use the restroom. We created spreadsheets and staggered video calls to make sure that someone who spoke English and could understand Hmong was always present.
However, for Southeast Asian and other minority communities, increasing healthcare access alone is not enough. Culturally and linguistically competent care is also necessary to ensure that our communities thrive. According to the 2019 American Community Survey, 32% of Southeast Asian Americans are limited English proficient (LEP), while only 8% of the general US population is LEP. It’s imperative that our healthcare services have robust language access support.
While Marny’s family prepared for her funeral, our grandmother was also hospitalized for COVID-19. To my family’s pleasant surprise, she survived. But because of her condition, she was transferred to one of two hospice care centers in the Twin Cities that accepted COVID-19 positive patients. There was no Hmong interpreter provided. Isolated, unable to speak English, and recovering from a speech impediment due to a prior stroke, our grandmother could barely ask for water and couldn’t even request food or to use the restroom. We created spreadsheets and staggered video calls to make sure that someone who spoke English and could understand Hmong was always present. My extended family and I were online with her from the moment she woke until she fell asleep. We weren’t allowed to properly grieve the loss of Marny before being forced to move on because our systems are not properly designed to help LEP and minority patients.
That is why Congress must move beyond just expanding healthcare but ensure that our healthcare services are culturally and linguistically competent. Supporting the Health Equity and Accountability Act (HEAA) of 2020 in the House and Senate is a start. HEAA would create more support for in-language services so that other families do not have to simultaneously be victim, survivor, and interpreter in times of crises. The bill would also disaggregate health racial data, allowing more targeted support of communities affected by specific illnesses.
This pandemic has irreparably harmed my family. I will never hear Marny laugh again or share another drink with her as we discuss the educational needs of Southeast Asian students. When I return to Minnesota, I will be greeted only by the empty seat that should have been reserved for her. But I know that if she were still alive, she would say that it is unconscionable for Senate leadership to prioritize a Supreme Court nominee to dismantle the ACA instead of providing COVID-19 relief to Americans. But she is not, so we must speak in her place and preserve her memory, not in our words, but in our actions and bend the arc of justice toward a more just and equitable future for everyone.
Kham Moua is SEARAC’s Director of National Policy. Email him at kham@searac.org.
Footnotes:
1 According to a recent analysis by the Kaiser Family Foundation, current federal support for COVID-19 testing and treatment for uninsured individuals do not provide “comprehensive access and protection from high medical bills as traditional insurance.” https://www.kff.org/policy-watch/limitations-of-the-program-for-uninsured-covid-19-patients-raise-concerns